Early Postpartum Breast Pain Relief
Week 1 Engorgement: What’s Normal, What’s Not, and How to Feel Better
Welcome to the first week of feeding your new baby—also known as the week your body suddenly realizes “Oh! The baby is here… time to make all the milk.”
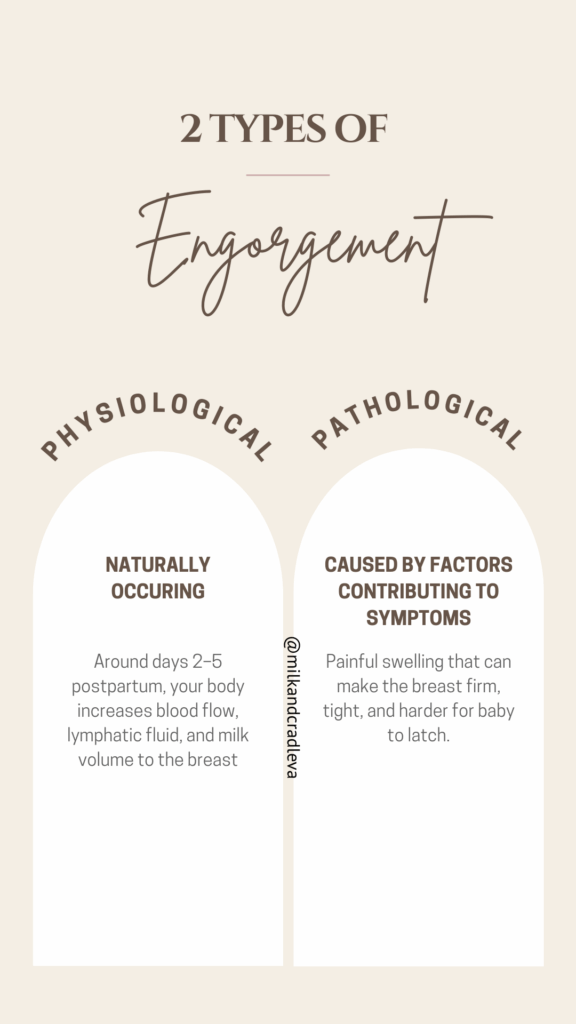
If you’re feeling full, heavy, warm, or even uncomfortably swollen, you are not doing anything wrong. In fact, this early engorgement is a sign your milk is transitioning beautifully from colostrum to mature milk.
But here’s the key:
We want to see engorgement come… and then go.
Persistent, painful, or worsening engorgement is a sign that milk isn’t being removed efficiently—which can make feeding harder for both you and baby.
Let’s walk through what’s normal, what needs attention, and what you can do to stay comfortable and keep milk flowing smoothly.
Why Engorgement Happens (and Why It’s Actually a Good Sign)
The goal is steady, comfortable milk flow—not constant pressure.
Tips for Managing Week 1 Engorgement (Based on the Academy of Breastfeeding Medicine Protocol)
The Academy of Breastfeeding Medicine’s updated protocol for breast pain encourages a physiologic, non-aggressive approach that protects milk supply while reducing inflammation.
Here’s what that looks like in real life:
✨1. Use Brief, Gentle Cool Therapy
Cold packs or a cool compress for 10–20 minutes can help calm inflammation and swelling. Do not place cool pack or compress directly onto the skin.
Think of it as icing a swollen knee to reduce inflammation and improve milk flow.
✨2. Soften the Areola Before Latching (Reverse Pressure Softening)
If the breast feels too firm for baby to latch, use light fingertip pressure around the nipple for 1–3 minutes.
This moves lymphatic fluid back into the breast and makes the nipple easier to grasp.
This technique is IBCLC-approved magic for those “my breast feels like a bowling ball” moments.
✨3. Avoid Over-Pumping (“Removing Just Enough” Is Key)
Pumping too much during engorgement teaches the breasts to make more, not less.
Instead aim for:
- Feeding on cue
- Pumping only to soften—never to empty—if baby is not latching well
Light hand expression for comfort is also helpful and keeps supply balanced.
✨4. Feed Frequently—Don’t Wait for Baby to Cry
Crying is a late hunger cue.
In week 1, baby may eat 8–12+ times per day—this is your supply-building rhythm.
Offer the breast at early cues:
- stirring
- hand-to-mouth movements
- rooting
- little “bird mouth” pecks
Frequent, comfortable feeds = less engorgement.
✨5. If Baby Is Not Latching—Protect Milk Removal Immediately
Any disruption in feeding can quickly lead to engorgement, plugged ducts, or reduced supply.
If baby isn’t latching well—or at all—you’ll need to help your body remove milk efficiently.
Examples of separation include:
- Baby in the nursery or out of the room
- Baby spending time with a caregiver
- A NICU stay
- A sleepy or disorganized feeder
- Baby who isn’t coming to breast due to tongue tie, jaundice, early birth, or recovery after delivery
During any of these situations, aim to:
- Hand express or pump every 2–3 hours
- Use a hospital-grade pump like the Spectra S1 if your baby is in the NICU
- Do a few minutes of gentle breast massage before expressing
- Keep expression sessions short and comfortable—this is about protecting supply, not draining the breast. A manual pump like the Lansinoh Manual Hand Pump can be beneficial for short term usage.
⚠️When to Call an IBCLC (International Board Certified Lactation Consultant)
You deserve to feel supported—not overwhelmed—during this transition.
Please reach out for a lactation consultation if you experience:
- Engorgement that does not improve after 24–48 hours
- Baby struggling or refusing to latch
- Nipple pain or damage
- Concerns about your milk supply
- Feeding sessions that feel unsustainable or stressful
An IBCLC can observe baby’s latch, assess feeding efficiency, and create a plan tailored to your situation.
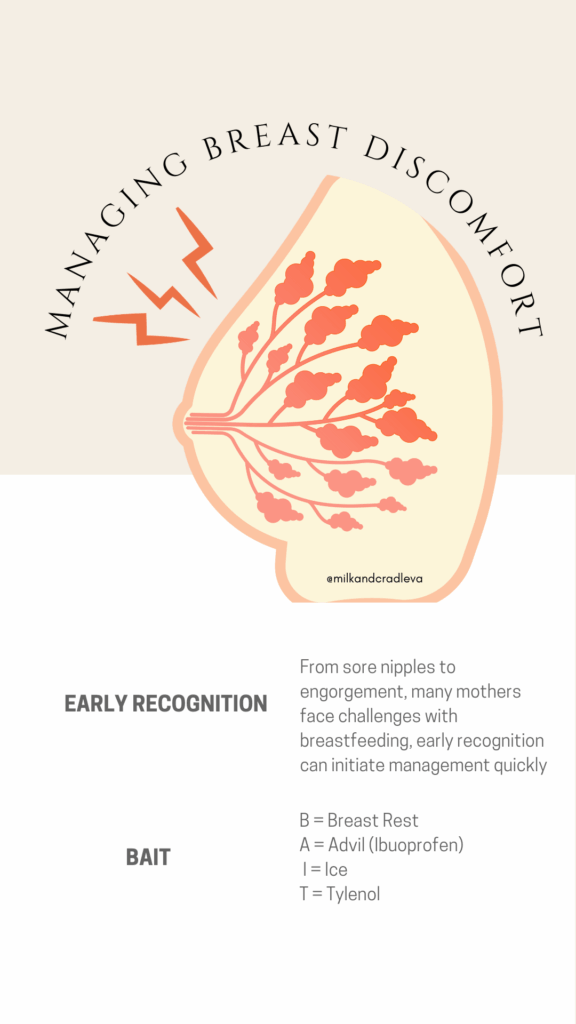
While connecting with an IBCLC consider starting the BAIT method of management for breast pain to prevent increased risks of mastitis.
Breast rest consists of only nursing and or pumping only as much as required to respond to baby’s demands.
Advil or Ibuprofen to manage inflammation
Ice between feeds and/or pump sessions for 30 min until symptoms improve
Tylenol for pain management
Contact your healthcare provider for medication dosages instructions if needed.
Ready for Help? Schedule Your In-Home, Office or Virtual Visit
Milk & Cradle offers insurance-covered lactation consultations for many families.
✔ In-network with Aetna commercial insurance plans
✔ Tricare-Certified Provider
✔ Other major plans may be covered with pre-authorization (United Healthcare, Anthem, Cigna)
✔ Self-pay options are available if needed
How to Schedule:
- Complete the contact card at the bottom of our home page
- You will be emailed with an intake questionnaire and further instructions
- Complete the brief intake forms so your appointment can be scheduled promptly.
Early support makes a tremendous difference—especially in week 1, when small adjustments can prevent major discomfort later.
You Don’t Have to Navigate Engorgement Alone
Engorgement is normal—but suffering through it is not required.
With the right approach and timely support, your milk can transition smoothly, baby can learn to latch comfortably, and feeding can become the bonding experience you hoped for.
If you’re feeling unsure, uncomfortable, or worried—Milk & Cradle is here to help.
You’re doing an incredible job, and you don’t have to do it alone.
Disclaimer: 1The information provided on this post is for educational purposes only and is not to be substituted for seeking professional care and support by a qualified provider. 2 This post contains Amazon Affiliate links and a small commission is earned from qualifying purchases.